
The neck in this case covers the cervical spine and all the muscles attaching to it, the area most people would call the neck, but also the upper back and shoulders. This is because the muscles and joints in these areas work so closely in conjunction with one another that any pain felt in these areas will involve one or many of these areas of the body. Neck pain can also occur with radiating arm pain, this is effectively the equivalent of sciatic for the neck/arm. Neck pain or stiffness can also lead to headaches.
There are 3 main types of musculoskeletal injury affecting the neck (excluding fractures) – muscle pain (myalgia), joint pain (arthralgia or arthritis) and nerve pain (neuralgia). Below is a discussion of each with links to the latest evidence based guidelines on treating these injuries along with what our clinic has to offer. At the bottom is a series of home exercises which are often helpful for these types of injury. Please bear in mind that without an assessment it is impossible to say if these exercises will be the correct ones for a specific case so if you have any doubts please consult your chiropractor first.
Muscle Pain – If the muscle is not torn/strained then this arises from “active” muscle trigger points, tight knots of muscle thought to occur due to fatigue either from overuse or poor conditioning. This means they can affect the very fit and the most sedentary. Generally described as a dull achy pain that gets worse towards the end of the day and possibly other symptoms such as numbness, tingling, pins & needles or weakness particularly in the arms. If they persist for a long time such as with a repetitive strain injury (RSI) they can become inflamed leading to more pain and referred pains around the head, face, arms & upper back depending on the location of the muscle trigger points.
Range of motion may also be affected leading to a feeling of stiffness and this may cause a person to alter the way in which they move in order to compensate for the discomfort, this can lead to other injuries or trigger points developing. Muscle trigger points are always associated with at least one stiff joint and vice versa joint pain/stiffness will always be associated with at least one muscle trigger point so for management of muscle pain see the information at the end of the next section on joint pain.
Joint Pain – Joints may be sprained or similar to muscle trigger points they can develop pain and stiffness over time from things like; poor posture, overuse, lack of use, injury, poor movement patterns or age related changes such as osteoarthritis. It is important to note that even though osteoarthritis is age related it does not mean that all 50 year olds are equal and when they are 70 they will show the same age related joint changes over a 20 year period.
Your joints, just like the rest of your body, respond to the stresses you put on them in combination with your inherited natural potential (genetics – blame or thank your parents!). Everybody shows some signs of osteoarthritis on x-ray over the age of about 20 this does not mean that your pain is due to osteoarthritis or your age and often there is more that can be done about it than just popping painkillers.
Joint pain will tend to be sharper than muscle pain and often feels as if something is “catching” on certain movements. It can also be a dull achy pain though and is often difficult to distinguish from muscle trigger points hence the need to look at and treat both. Many people will find changes in the weather affect their joint pains. Often holidays in hot countries will reduce or even completely relieve joint pain which quickly builds up again upon returning to the UK.
It is not clear why weather changes arthritic symptoms, it may just simply be the heat loosening up the muscles around the joints (and increasing blood flow) similar to warming up before physical activity or there may be other environmental factors such as pressure changes within the joint fluid or changes in vitamin D levels affecting the immune system (which controls inflammation). Current advice to help manage this kind of arthritic pain is to bugger off to Spain for the rest of your life…..if only that were true!
In all seriousness exercise and a healthy diet are the obvious ones but other dietary advice can be misleading. The latest cochrane reviews on dietary aids for osteoarthritis suggest arnica may be as effective as NSAID’s such as ibuprofen but surprisingly arnica may be more harmful. It is unclear if capsicum is effective but comfrey extract gel probably does improve pain so I would currently recommend trying that first if you are looking for non-pharmaceutical alternatives. Chondroitin, alone or in combination with glucosamine, may also be beneficial in the short term at least.
What can we do for you? A short course (usually 4-8 treatments) of manipulation or mobilisation combined with some form of soft tissue therapy like trigger point therapy or instrument adjusted soft tissue mobilisation (IASTM – basically graston without the trademark!) will relieve pain and restore mobility in most cases of joint or muscle pain. Other treatments like dry needling (a more specific form of acupuncture) and rocktape, which is a brand of kinesiotaping that is commonly seen on sports people to help keep their muscles flexible and reduce swelling. Also whilst it cannot cure osteoarthritis manual therapy is one of the most effective ways of managing the symptoms along with exercise which we will also advise on.
Also, manipulation of the thoracic spine has been shown to be at least as effective as manipulation or mobilisation of the neck or C/T junction, even in a single session.
Long term management of any neck injury will depend on how much you avoid or reduce the aggravating factors and how often you practise the beneficial exercises. Another good way of managing the symptoms is to have periodic treatment every few months instead of letting the problems build back up again, chiropractors call this “maintenance” treatment and it is similar to what dentists offer to look after your teeth or having your car serviced before breakdown occurs.
What can you do for yourself? See the exercises at the bottom of this page. The most important thing is keeping the neck moving and having good posture most of the time. The way your neck lies in relation to your pillow is also a key aggravating factor for neck pain. There is no right answer to the question which is the best pillow. Even the expensive orthopaedic pillows will not help you if you don’t put them in the right position and keep them there throughout the night. Try to find a pillow arrangement that leaves your neck in a relaxed position during the night, usually it is best to sleep on one side or your back, definitely not on your front as this will lead to neck pain.
What does the evidence say? The main clinical guidelines in the UK are produced by NICE and they are updated every few years. Currently NICE do not have any recommendations for neck pain. However other large scale systematic reviews have been carried out and they support manual therapies such as manipulation/mobilisation in combination with exercise advice and soft tissue therapies for up to 9 treatments over a 12 week period.
Nerve Pain – This is where things get a little more complicated because the real problem is identifying what is causing the nerve to be irritated. It may actually be tight muscles like the scalenes or pectoralis minor which would then follow the muscle pain section above and be referred to as thoracic outlet syndrome (TOS). Nerves can be compressed due to degeneration of the spine over time reducing the size of the holes that nerves exit the spine. In the early stages this can easily be treated similar to the way described in the joint pain section above.
In later stages this may become a condition known as stenosis. This is particularly important if it ever reaches the stage of spinal cord compression. This is referred to as cervical spine myelopathy (CSM) and will lead to progressive leg weakness among other symptoms. Depending on the type of nerve compression causing the stenosis it may respond to manual therapy and exercise but some cases (CSM) will require surgery, your chiropractor will be able to advise you when this is necessary.
The other common cause of stenosis is a disc bulge. The discs are specialised forms of connective tissue found between the surfaces of each spinal vertebral complex (between each pair of bones). They degenerate naturally over time but also as with the rest of the body the speed of degeneration depends on what you do….things like prolonged sitting or standing have been associated with greater disc degeneration as has smoking, being overweight and forward head posture particularly when reading, watching TV or working on a computer.
Most disc bulges occur posteriorly and laterally (poking out backwards and to one side) and may trap or inflame the nerve root that exits at that level of the spine leading to nerve pain that radiates along the course of that nerve (radiculopathy). The most common vertebral levels affected in the neck are between C5/6 and C6/7 both of which have nerve roots that form part of the collection of nerves running down the arms called the brachial plexus. These nerves form into 3 distinct nerves (median, radial & ulna) running down the arms which give off branches of nerves to different areas of the arms. Carpal tunnel symptoms can be coming from the neck therefore not just the wrist.
The greater the level of nerve compression the more severe the neurological symptoms will be (not necessarily pain). Pain can be just inflammatory and does not mean the nerve is being compressed. Sensory symptoms such as numbness, tingling and pins & needles will occur with mild nerve compression. With greater nerve compression the muscles will start to lose nerve supply leading to muscle weakness. This is a more serious sign as prolonged or rapidly increasing muscle weakness may lead to permanent deficit. The worst of these cases will require surgery.
What can we do for you? Well in most cases the same treatments that help with muscle and joint pain also help with nerve pain. This is most likely because improving your mobility and posture will reduce the stress on the disc/nerve and those treatments also have a pain relieving affect. The main difference is these injuries take longer and usually require more treatment (8-12 treatments).
Acupuncture can also help with pain relief. There are specific exercises that often help too, see below for a list of the commonly helpful ones but remember if it is making the arm pain worse and travel further down the arm then it is probably not helping. Things that help to localise the pain closer to its origin in the neck (centralisation) are likely helping. Things that increase the pain further away from the origin of pain towards the fingers are likely hindering recovery (peripheralisation).
What can you do for yourself? A key part of managing nerve radiculopathies is reducing the daily irritation to the nerve so the inflammation can heal any tissue damage and then settle down. Therefore reducing inflammation (but not stopping it altogether) will help control pain (ice for 10 mins 3-4xday) and avoiding or reducing any aggravating postures will stop inflammation building up. For example try taking regular breaks from sitting if you have a sedentary job and if you have a job involving lots of bending/lifting then make sure you do it with good technique and limit how much of it you have to do.
Nerve inflammation can be very painful and can take 2-6 months to recover so it may also be advisable to seek pain relief from your GP or pharmacist. For more self help see exercises below.
What does the evidence say? The NICE guidelines do not have a guidance report on neck pain, traction can help as can manual therapy. Steroid injections will reduce pain for up to 1 month by preventing your immune system from producing inflammatory cytokines, however this will also reduce the healing process and in most cases the pain returns and is not better after 12 months.
Home Exercises: The level one exercises are for beginners who want to reduce their current neck pain and also reduce the chances of it returning in the future. The best results will likely be obtained at levels 2 and 3 but you should not progress levels unless you have really mastered the previous level.
Level 1 – Start with improving breathing patterns & mobility of the neck, shoulders, upper and mid back (thoracic spine). Also at this level try and learn the basics of deep neck flexor strength and shoulder retraction.
Breathing patterns: If you can make your diaphragm do most of the work for you during normal levels of breathing then your scalene muscles (a major contributor to neck pain) should get less fatigued and cause fewer neck & arm problems. Begin laying on your back with one hand on your tummy, one hand across your upper chest. The aim is to feel the expansion of your lower ribs & stomach and use the hand on your chest to feel if any expansion occurs there (it should not).

In order to get the feeling for the two styles of breathing try taking 5 deep breathes through the diaphragm/abdominals followed by 2 deep breathes through the neck/chest. This latter method is the one you want to avoid most of the time but it can help some people to be aware of when they are breathing incorrectly by practising it a few times. Try this for a few weeks and when you feel you don’t need your hands to check try just breathing through your diaphragm only for at least 1 minute before you go to sleep each night. Use this breathing technique through all the exercises that follow.
Deep Neck Flexors: Located under your chin these small muscles are well positioned to control the weight of your head tipping in front of your shoulders. The simplest way to start strengthening these muscles is to lay on your back with a small pillow under the neck (not head). Then try and tuck your chin as if you are pulling it straight down towards the floor giving yourself a “double” chin. The aim is to use the deep neck flexors and keep the larger muscles around your neck relaxed so it should be a small movement.
 The next stage is to do the same thing seated or standing as in the picture above. Try doing this in front of a mirror to begin with so you can see if you are tensing the bigger muscles in your neck by mistake. You will probably feel a stretch around the back of your skull (occiput) as you do this.
The next stage is to do the same thing seated or standing as in the picture above. Try doing this in front of a mirror to begin with so you can see if you are tensing the bigger muscles in your neck by mistake. You will probably feel a stretch around the back of your skull (occiput) as you do this.
Brugger posture relief: Once you have mastered the chin tuck sitting or standing you can add some extra stretch to the upper back and shoulders by squeezing your shoulder blades together and down towards your buttocks. Keeping your elbows in against your side and your palms facing up, rotate your forearms/hands outwards to increase the stretch across your chest.

Pec stretch: The pec muscles across your chest are probably the biggest culprits in holding you in a rounded shoulder posture, therefore they need to be stretched regularly even if they don’t actually hurt. Standing or sitting upright clasp your hands behind your back and lift your arms as far up behind your back as you feel comfortable without leaning forward. If you are struggling to avoid leaning forward do it facing a wall.

Neck stretches: Best done with holding a table/chair to keep your shoulders down so you really are stretching your neck not just lifting your shoulders. Always keep the chin tucked and do not roll your neck, treat each stretch as a separate movement. Firstly move one ear towards the same shoulder keep facing forwards. Repeat the other side, 30 second holds on each. Next rotate your head to look over each shoulder, hold for 5 seconds each side and move slowly side to side.
Level 2 – You should continue working on the level 1 stretches as a daily routine added to that at least a couple times per week you should try and strengthen the mid back muscles like the rhomboids and mid/lower traps. Pulling exercises such as rows, pull ups or pulldowns will help with this as long as you maintain good posture throughout so your chin should stay tucked and your shoulders should stay held down and back.
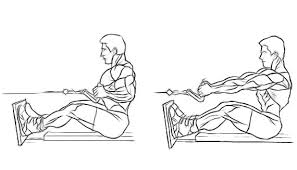
Seated Row: All gyms should have a seated row machine but with an elastic band or towel at home the same exercise can be performed to a reasonable degree. Sit upright with a slightly arched lower back and tense tummy muscles throughout, there should be no jerking of the trunk. Keeping your shoulders down and elbows close to your sides pull the bar/band/towel etc back until your hands are by your sides. If you are using a towel or something similar that doesn’t stretch then just hold the pull for up to 10 seconds the right muscles will still be working.
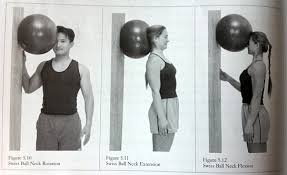
Neck flexions: Using a towel or cushion (or swiss ball as in picture below) between your forehead and a wall you can strengthen your deep neck flexors. Remember to keep the chin tucked as you try and push your forehead into the towel/cushion focussing on the majority of the effort coming from the deep neck flexors. As you can see in the picture below if you change your position you can repeat the exercise to strengthen the rest of your neck. Start at 10 repetitions and build up to 20-30 repetitions over time.
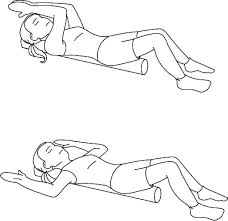
Foam Roll: Buy a long (90cm) foam roll and you can lay length ways on it supporting your buttocks and head. 2-3 minutes of this will gently stretch and mobilise your thoracic spine and also your pec muscles if you allow your arms to rest out to the sides as in the picture below.
Level 3 – Most people should get enough out of levels 1 & 2 after 2-3 months of regularly doing those exercises. If you want to push on further though here are some other options.
McGill Curl up: Don’t ever do sit ups they are bad for your back and there are plenty of better options for strengthening your tummy muscles. The same goes for leg raises in my opinion although I do accept that if your core strength is at an elite level you could do leg raises with proper form. But to be honest if your core strength is that good what do you need to do leg raises for anyway!
McGill curl ups are crunches where your tummy muscles and deep neck flexor muscles are getting strengthened at the same time (if your form is good!). Start laying flat on your back with one knee bent and hands in the small of your back. Keep you chin tucked and crunch up using your tummy muscles until your shoulders begin to lift off the floor. Relax back down and repeat you should not feel any pressure on your hands from your back as your lower back should not move.

Wall angel: Stand with your feet shoulder width apart and slightly away from a wall. Sit your butt back onto the wall with your head and shoulders also touching the wall. Raise your arms to shoulder height and bend your elbows to 90 degrees. Your hands and elbows should also now be touching the wall. Keeping all those points of contact with the wall (head, elbows, shoulders, upper back & buttocks) try and flatten your lower back against the wall.
If you are flexible enough to flatten your back against the wall without losing the previous points of contact then you can try keeping that new position and rotating your shoulders so your hands move down towards the wall below your shoulders. Repeat the whole thing 5-10 times to improve mobility.


You must be logged in to post a comment.