
Knee pain is the second most common area to suffer a musculoskeletal injury behind the low back. Yet the knee is just a simple hinge joint, unless you’re doing lots of jumping or sudden changing of direction it should not take excessive stress.
Many believe that knee issues are the result of either hip, ankle/foot or core/pelvic dysfunction, so they overload their knees (as a hinge joint it has less ability to compensate for dysfunctional movements) leading to injuries such as patellar tendonitis/bursitis, iliotibial band syndrome, patellofemoral pain syndrome, knee osteoarthritis, meniscus tears, collateral ligament sprains and ACL/PCL sprains.
Below is a brief run through of these conditions and what we and you can do about them. For more specific advice please see a manual therapist like a chiropractor, physiotherapist, sports therapist or osteopath. Preferably one who specialises in rehabilitation exercises.
Knee osteoarthritis/meniscal tears: Meniscal tears can be due to traumatic injuries, but they are also commonly the result of knee joint degeneration, hence why they are grouped here with knee osteoarthritis (OA), aka degenerative joint disease (DJD) of the knee. Sometimes meniscal tears will require surgery but conservative therapy such as manual therapy and exercise should always be tried first.
Degeneration of the knee will occur quicker than the natural ageing process if you have poor hip/knee/ankle/foot biomechanics and if you are overweight. Strengthening the hip (mainly glutes), knee (quads, hamstrings and calves) and core muscles whilst reducing excessive tension in the quadriceps/hamstrings and calves will lessen the wear and tear on the knee and pain.
What does the evidence say? According to a review by Skou and Roos (2019) there are more than 50 randomised controlled trials confirming the benefits of exercise for reducing knee pain and dysfunction with OA/DJD. Land based exercise is better than water based exercise, although if pain is too great on land then water based is a reasonable alternative. Patients should begin with an exercise program (supervised is superior to at home) and weight loss (if they are overweight). For those not improving after 12 weeks at least one course of manual therapy and/or a knee or foot orthosis should be offered. Injections, painkillers and surgery (total knee replacement is one of the best pain relievers but the cost and risk of surgery, and good performance of exercise comparison groups make surgery a last resort) should only be offered if the previous methods have failed. The best results from exercise are seen in supervised exercise programs lasting at least 12 weeks and occurring at least 2 times per week. If you want to use painkillers topical (gels/creams applied to the skin) are safer and as effective as oral (tablets/syrups taken by mouth) painkillers ie NSAIDs and Paracetemol.
Strength training with gradual progression of difficulty is important, so exercise should not just include walking, cycling or swimming (aerobic exercise). Exercises should not just focus on the knee and quadriceps, although in patients with a BMI over 30 quad dominant exercises do show a greater effect than other exercises.
The bronfort report supports the use of manipulation/mobilisation, massage and exercise for knee osteoarthritis. Cochrane reviews support the use of exercise for knee osteoarthritis. NICE guidelines support the use of exercise but their pain medications guidance is currently under review due to concerns about possible side effects.
What can a therapist do? Exercise, patient education and weight loss should always be in conjunction with manual therapy not manual therapy alone. Skou and Roos (2019) suggest that manipulation/mobilisation of the pelvis/hips and ankles/feet can help to improve reduced mobility that leads to knee dysfunction and also reduce knee pain in the short term (regular sessions ie once a month or every 2-6 months called “maintenance” therapy will be needed as manual therapy does not “cure” OA/DJD). Soft tissue therapies such as deep tissue massage, trigger point therapy & instrument assisted soft tissue manipulation (IASTM) applied to the quadriceps, glutes and hamstrings in particular can help to reduce unwanted tension on the knee joint and significantly reduce pain in my clinical experience (but evidence is currently lacking to support this). Vickers et al. (2018) suggest that acupuncture is generally more effective than placebo for reducing pain in knee OA and the effects can last several weeks/months.
What can you do for yourself? Regularly ice the knee for 10 minutes at a time. Daily stretches of the quadriceps at least. Strengthen the leg muscles in general but specifically the glutes, quads and hamstrings are most important. Depending on pain levels you may need to take pain medication but bear in mind taking these long term will cause significant side effects to your general health so why not try comfrey gel.
One of the other major contributors to knee degeneration is obesity so if you are overweight and getting knee pain here is another good reason to eat healthier and do more exercise.
Patellar tendonitis/bursitis/Iliotibial band syndrome/Patellofemoral pain syndrome: The patellar tendon should help concentrate the pull of the 4 quadricep muscles into one straight line force. The patellar (knee cap) is encased within the tendon. If you kneel excessively then you may develop pain & selling in the fluid filled pads (bursa) that protect the front of the knees this is termed bursitis. If the tendon becomes inflamed from overuse (or lack of strength to deal with the demands placed on it) of the quadriceps this is termed tendonitis.
Iliotibial band syndrome is when the fascia along the outside of the thigh is pulled too tightly by the glutes (specifically tensor fascia latae) which begins to cause a repetitive strain injury to the outside of the knee. It is associated with poor hip biomechanics, common in runners.
Patellofemoral pain syndrome is really knee pain which doesn’t quite fit any of the other more specific diagnosis. No tissue is obviously damaged so the general area is described as painful. It is also caused by poor hip biomechanics, hopefully you are noticing a pattern!
Your quadricep muscles should be loose enough to comfortably sit back onto your heels with your shins on the floor. Your glute muscles should control the line of your thigh bone so that the knee operates as a hinge without rotation or lateral overpressure. This is harder for females due to the natural wider angle of their hips (Q angle).
What does the evidence say? Taping only reduces pain whilst its on the leg and for a short time afterwards. NICE do not offer guidance on tendonitis/bursitis. The Bronfort report supports the use of manipulation/mobilisation and exercise for PFPS. Cochrane reviews support the use of exercise in the management of PFPS. Ferber et al. (2015) showed that a 6 week exercise program for the hips and “core” was just as good at reducing patellofemoral pain as a knee exercise program, in fact the patients found significant improvement 1 week earlier in the hip/core group, further supporting the idea that PFPS is related to hip/pelvic dysfunction.
What can therapists do for you? Manipulation/mobilisation of the pelvis/hips and ankles/feet can help to improve reduced mobility that leads to knee misalignment. Soft tissue therapies such as deep tissue massage, trigger point therapy & instrument assisted soft tissue manipulation (IASTM) applied to the quadriceps, glutes and hamstrings in particular can help to reduce unwanted tension on the patellar tendon.
Kinesiotaping can help encourage correct biomechanics of the knee and also reduce excessive muscular tension. To gain the full benefit of taping you need to do your exercises a lot whilst wearing it.
What can you do for yourself? You need to practise regularly exercises that emphasise good hip/knee biomechanics and also stretch excessively tight muscles like the quads every day. For inflammation reduction ice for 10 minutes at a time a few times per day will help. For tendonitis eccentric stretches are particularly important, see below. For bursitis if you have to keep kneeling a lot then try using knee pads.
What does the evidence say? Taping only reduces pain whilst its on the leg and for a short time afterwards. NICE do not offer guidance on tendonitis/bursitis. The Bronfort report supports the use of manipulation/mobilisation and exercise for PFPS. Cochrane reviews support the use of exercise in the management of PFPS.
Collateral & Cruciate ligament sprains: Knee ligaments are usually sprained by some sort of trauma where the knee is exposed to excessive shear forces either to the sides (collateral ligaments) or forwards/backwards & twisting (cruciate ligaments). There is an anterior and posterior cruciate ligament hence the more common terms ACL/PCL.
Initial care depends on the level of sprain, more severe sprains will require surgery for less severe sprains just follow the PRICE protocol. Once enough tissue healing has occurred manual therapy can help to reduce any stiffness from the immobility during healing. Exercise must be gradually progressed over several months to regain full ligament function without re-injuring. This is specific to each case so will not be included in the general exercises below, you should consult your chiropractor for guidance.
Exercises for knee pain (excluding ligament rehab) – As mentioned above ligament rehab needs to be progressed slowly on a case specific basis but knee osteoarthritis, patellar tendonitis etc can all benefit from the same sort of exercises based mostly on glute strength/ quad stretching.
Eccentric Knee extensions: This one is for patellar tendonitis only and you should focus on this exercise before moving onto the others (if you have patellar tendonitis) only when the pain is significantly improved.
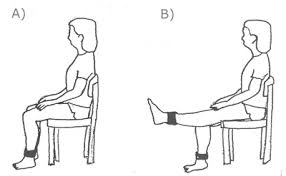

Muncie Exercises: These are very simple knee exercises to encourage the correct tracking of the knee cap through the front of the knee joint. Simply roll up a towel and place it under the thigh. Focus on contracting the inner part of the quadricep nearest the knee (vastus medialis) as you straighten the leg, lifting the foot off the ground. This exercise needs to be performed as part of a squat type exercise to become beneficial in the long run, this is just an easy way to get started.

Sit-to-stand: Basically a squat but easier. Start from a seat that puts your hips above your knees, higher the seat, easier the exercise. Thinking about the muncie exercise above also focus on keeping your knees behind the tip of your toes (use your hamstrings to hold knees back) and drive your heels down into the ground using predominantly your glutes to push you to standing. Your knees should also not move closer together during the movement, they should remain hip width apart. As you get more confident try lower seats for a greater challenge eventually aiming for a position like that shown below.

Split squats: A single leg version of the squat described above. Same rules apply, front knee behind toes, dont’ let the knee move in or out and control the movement through your hip (glutes). Avoid the temptation to use your back leg for any help other than just balance. If your back quad is burning more than your front glute you are not doing it right!

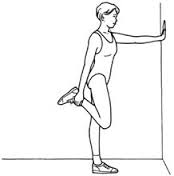
Stretch those quads and hip flexors: Below are some pictures of quad stretches in progressive order of difficulty. By the time you get to the last one you shouldn’t have any knee pain!





You must be logged in to post a comment.