
The hip is an area that causes some confusion diagnostically. Pain coming from the buttock muscles is often termed hip pain but realistically this is best thought of as an extension of low back pain rather than pain coming from the hip joint. This section predominantly deals with 2 types of hip pain, osteoarthritis (OA) of the hip and hip bursitis. They are very different conditions so do not confuse the management of one with the other if you want the best results.
Degenerative hip disease (osteoarthritis) – At its worst this will require a hip replacement, some surgeons will make you wait until the pain is unbearable before they will operate however so even severe cases need to have some sort of management plan for the pain. Unfortunately this approach of making you wait longer for a replacement will inevitably lead to other joints in your body such as your knees also needing surgery due to the way you will be forced to compensate when walking for the groin pain from the hip.
The early signs are decreased range of motion of the hip, groin pain and “giving” way of the hip when walking. In the early stages there is plenty you can do to reduce the chances of needing surgery. In the later stages you will likely need to resort to regular pain medication to get through the day. There are exercises at the bottom of this page that can prevent the need for surgery but you also need to look at the factors in your life that may be causing the degeneration and reduce/avoid those for the best results.
What can we do for you? Manipulation/mobilisation of the hip has been shown to reduce the symptoms of hip osteoarthritis better than exercise therapy over the course of 9 sessions. Exercises or further periodic treatment sessions can then be used to maintain the results over a longer period. Acupuncture is as effective as exercise for pain relief.
What can you do for yourself? Walking and swimming are often suggested as good exercise for hip OA although more than a few miles walking and your symptoms will likely worsen. Regular short walks with a good stretching program at the end of the walk would be a better option. Cycling is also likely to help keep the hip mobile. There are some stretching/strengthening exercises shown below.
What does the evidence say? The Bronfort report suggests manipulation/mobilisation of the hip is helpful. NICE do not offer any specific guidance on hip OA and manual therapy/exercise. Cochrane reviews support the use of land based exercises for pain reduction.
Hip Bursitis: This has little to do with hip OA. It is an overuse injury similar to tendonitis and can affect other joints too like the shoulder, knee and elbow. The initial stages will be periodic burning/aching in the buttocks and lateral thigh. If the aggravation (RSI) continues then the pain will become more constant and it will be painful to lay on that hip. If it becomes severe enough it may require steroid injections to give temporary pain relief although you will still need to modify aggravating factors with either manual therapy or exercise for longer term relief.
What can we do for you? Hip bursitis begins as a repetitive strain injury to the hip stabilising muscles in the buttock. Therefore soft tissue therapy such as stretching, massage and IASTM as well as kinesiotaping can all help to reduce symptoms. Manipulation/mobilisation of the pelvis is also helpful as this is usually too stiff forcing the muscles into overuse. Acupuncture (dry needling) can be helpful for pain relief. The most important long term factors are identifying the movement patterns that are causing the RSI and giving appropriate exercises to correct for these.
What can you do for yourself? Getting the inflammation under control is key to reducing pain so ice the hip for 10 mins at a time several times a day. You can do stretches, as shown below, for the hip stabilisers and general core strengthening exercises will also help reduce the load on those muscles, these can be found on the back pain page.
What does the evidence say? NICE have reports on shock wave therapy and distal iliotibial band lengthening but neither report shows any good quality evidence of effectiveness. There are no cochrane reviews completed on hip bursitis. The bronfort report does not mention hip bursitis. There are some systematic reviews available on pubmed but at this stage they are of limited quality. They do however suggest that surgery is more effective than steroid injections, home exercise and shock wave therapy. No large scale studies on manual therapy for hip bursitis have been published as yet.
Exercise for hip degeneration/osteoarthritis – The effectiveness of these exercises will depend on the stage of the problem you are at. They are least likely to be effective for the more severe cases. It is also important to do general core stability and lower limb mobility exercises so see back pain page for these.
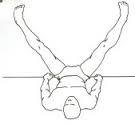
Short adductor stretch: To stretch these muscles effectively keep the knee bent, you can stretch both sides at the same time by just sitting with your elbows pushing your knees apart.

Long adductor stretch: This time keep your legs straight to bring the long adductors on stretch. Doing it the way shown in the picture should allow gravity to do the stretching for you.
Glute stretch: Laying on your back or seated you can simply pull one knee towards your other shoulder until you feel the stretch in your glutes.

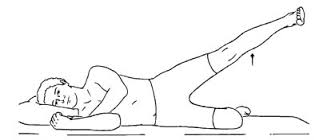
Side lying hip abductions (Clams): Before you consider trying the squat or its single leg variations like the step up you can try and build some endurance in your hip stabilising muscles. Keep your knees bent with your feet touching each other. Without twisting your trunk raise one knee away from the other.
Hip traction/mobilisation: Gently stretching the hip joint with some mobilisations can help improve your hip mobility. If you have an elasticated theraband you can add some traction to the hip as shown below. Just move the knee up & down and through some circular motion as long as it is pain free.

Exercises for hip bursitis – General core stability exercises will help but reducing glute muscle tension is the main aim of stretching. If the condition has reached the level of tendonitis/bursitis then you may need to do eccentric stretches. For standard glute stretching see above.
If the pain is not too bad then you can do some general glute strengthening exercises to prevent the hip from becoming irritated, see this video for example. If the pain is too much though you will have to use stretches like the ones below to try and reduce the pain first.
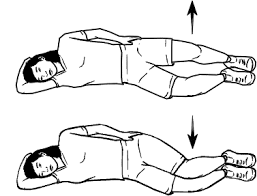
Eccentric glute stretch: The key to eccentric stretching is to only do the slow,controlled lowering part, do not use the glutes to lift the leg back to the start position (shown below). If you have a partner to help you lift the leg that is easiest but if you have to do it yourself bend your knee and hip up towards your chest, use your arm to pull your knee higher and then straighten your leg back to the start position. From this position slowly lower the leg back to the floor.
Hip aeroplanes: This one will be tricky to do if the pain is severe but in mild cases this is perhaps a more “functional” way of strengthening the hip stabilisers and if you put your other foot down between each rep to stand up again then you could just repeat the lowering part slowly for an eccentric stretch. The key to it is to use the glutes to control hip rotation and not twist your trunk at all (easier said than done).


You must be logged in to post a comment.